Wize University Physiology Textbook > Somatic Nervous System (SNS)
Motor Control - The Brain
Popular Courses
MCAT
General Course
DAT
General Course
Intro to Physiology
University Study Guides
PHYSIOL 1021
Western University
PHYSIOL 2130
Western University
Intro to Physiology
University Study Guides
PSL300H1
University of Toronto
PHYSL 210
University of Alberta
PHGY 210
McGill University
PHGY 215
Queen's University
KNES 259
University of Calgary
PHGY 216
Queen's University
BIOL 273
University of Waterloo
BIOL 260
University of British Columbia
PHYSIOL 3120
Western University
KNES 260
University of Calgary
BIOL 116
Case Western Reserve University
PPT 301
University of North Dakota
ANAT 212
McGill University
HTHSCI 2FF3
McMaster University

0:00 / 0:00
The Motor Cortex
It actually consists of 3 main divisions
- Primary Motor Cortex - see below
- Premotor Cortex - diverse functions including muscle preparation/orientation before actual movement happens
- Supplementary Motor Cortex - responsible for control of movement

- areas of the brain which initiates voluntary muscular activity
Watch Out!
This concept is the same as we see in the primary somatosensory cortex, but its not the same structure! This one is not for sensory signals, but rather for MOTOR signals.

- As in the somatosensory cortex, some areas of the body may show different levels of representation. This is because the density of motor units in that area of the body is larger.
- motor cortex is located on the PREcentral gyrus
- somatosensory cortex located on the POSTcentral gyrus
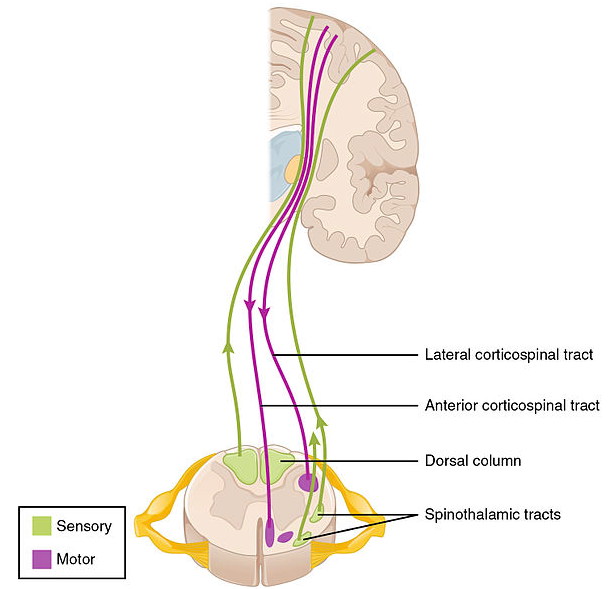
Corticospinal Tract
- neuronal tract which leaves the motor cortex and travels to the spinal cord
- The dorsal lateral tract is “crossed” (left brain affects right side of body) and controls fine and gross motor movement
- The ventral medial tract is “uncrossed” (primarily affects the same side) and affects gross motor movement
- both images below are showing the same thing. The first diagram shows the location of each part in the spinal cord really well, while the second picture better depicts the connections in the brain and the number of neurons (its not a single neuron leaving the brain)

How is the precentral gyrus represented?
0:00 / 0:00
Brain Plasticity
- plasticity is the ability of the nervous system to change its properties to adapt..
- No one has the exact same somatosensory and motor map because its layout is influenced by your development, experience, and physical injuries.
Changing the motor map
- Experience dependent plasticity - when neurons are repeatedly activated together in response to something, the connection between them (i.e. the synapse) gets stronger.
- When things aren't used, the area of the cortex coding for them is taken over by something else.
- ex. when someone loses a limb, its often that they feel fantom limb (they feel the hand they lost) or when touched in another place on the body (ex. hip), they feel sensation in the limb they no longer have. This is an example of changes happening in the brain.
0:00 / 0:00
What would likely happen at the end of one year if a basketball player performed 100 free throws every day?
- The player would have more motor units coded to perform that movement
- The player would perform a free throw exactly the same every time
- The player would strengthen the connections of the reflex arc associated with that movement
- The players motor cortex would have a larger area given to the motor neurons excited when performing a free throw.
1 - the number of motor units stays the same. This is the nerves in the body innervating the muscles.
2 - There is always variation in movement - its never exactly the same every time. There is still place for error.
3 - this movement is not a reflex, so it doesn't use a reflex arc.
4 - CORRECT
0:00 / 0:00
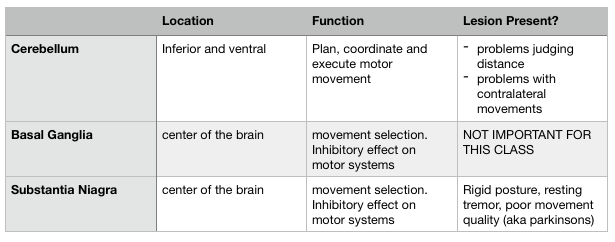
Cerebellum
- located at the bottom/back of the brain (dorsal/inferior)
- main role is in movement
- 2 major functions we need to know:
- Planning motor movements and coordination
- Motor execution
- the basic idea of the cerebellum is that its a monitor for muscle movement. The motor cortex tells the cerebellum what movement its planning on doing, then the cerebellum makes sure its carried out properly. If its not, it tells on the body to the motor cortex so the problem can be fixed.
- ANALOGY: If you were ever part of individual sports like dancing or you played an instrument such as the piano, you might be familiar with assessments. Basically you prepare a routine for the level you're at, then you go to an assessment and the person watches tells you if you performed successfully at that level or not. Usually athletes or musicians do this to pass levels and get better. The cerebellum is much like that assessment person. They know what level/activity you're supposed to be executing and they make sure its done properly. If not, your couch will be informed and you might have to try that exercise again!
- said another way: the cerebellum compares the intentions of the motor cortex with what actually happens in the muscles, then reports back.
- big take away from below image: the cerebellum is compartmentalized and each area has a different function
- you do not need to know the locations of all these things.

Cerebellar Damage
- damage to the cerebellum causes problems with...
- motor control (specifically its execution)
- judging distance (aka dysmetria)
- rapid movements. Especially those using opposing sides of the body
- these problems show all over the body
- could have a problem in the hand when you reach for something, or you could have a problem walking as it effects your legs
Basal ganglia and Substantia Nigra
- both located in the center area of the brain
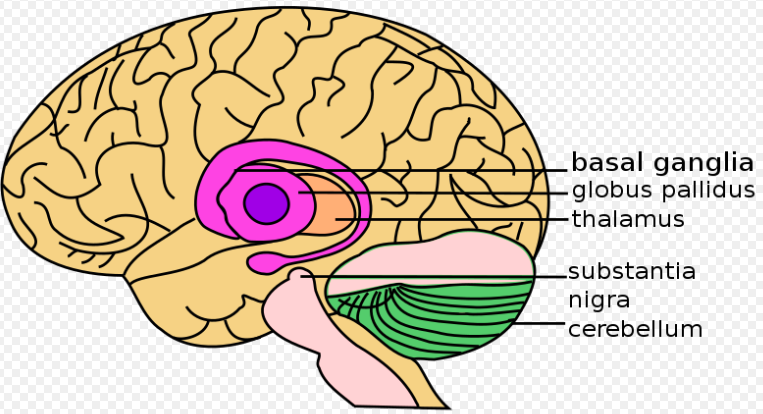
- they work with the cerebellum to control movements
- they are involved in selecting movements, deciding actions and planning of actions
- main function is to exert an inhibitory influence on motor systems. Basically they are trying to keep movements under control.
0:00 / 0:00
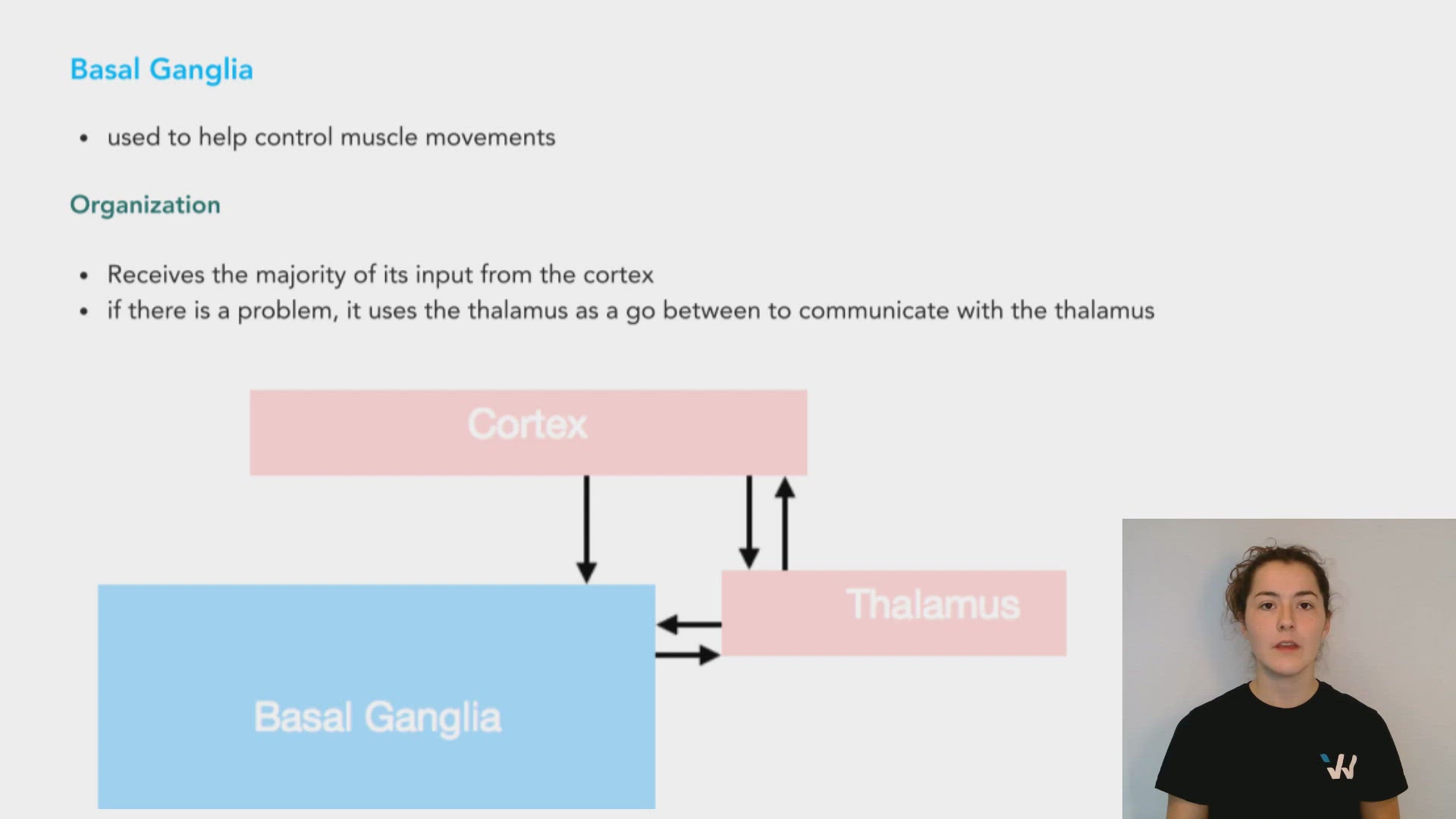
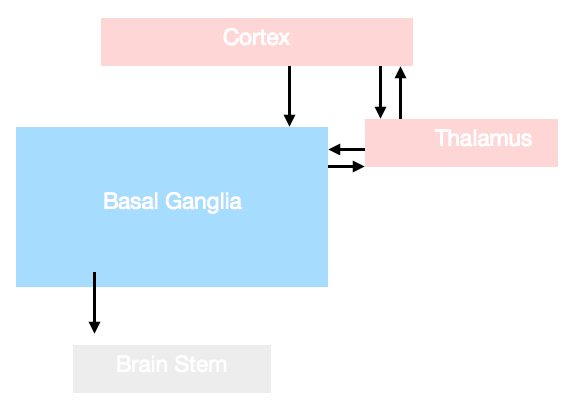
Basal Ganglia
- used to help control muscle movements
Organization
- Receives the majority of its input from the cortex
- if there is a problem, it uses the thalamus as a go between to communicate with the thalamus
0:00 / 0:00
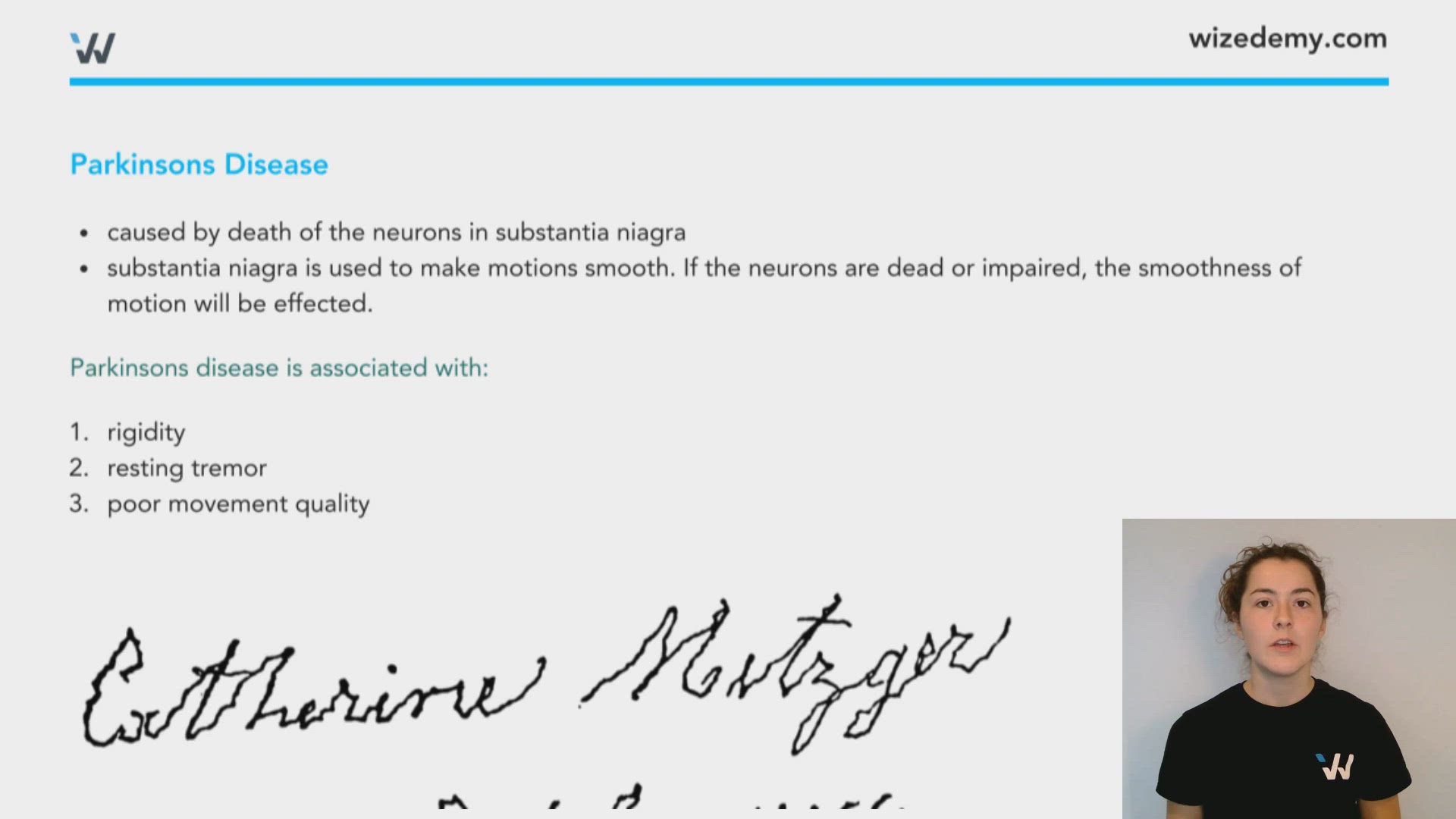
Parkinsons Disease
- caused by death of the neurons in substantia nigra
- substantia nigra is used to make motions smooth. If the neurons are dead or impaired, the smoothness of motion will be effected.
Parkinsons disease is associated with:
- rigidity
- resting tremor
- poor movement quality
0:00 / 0:00
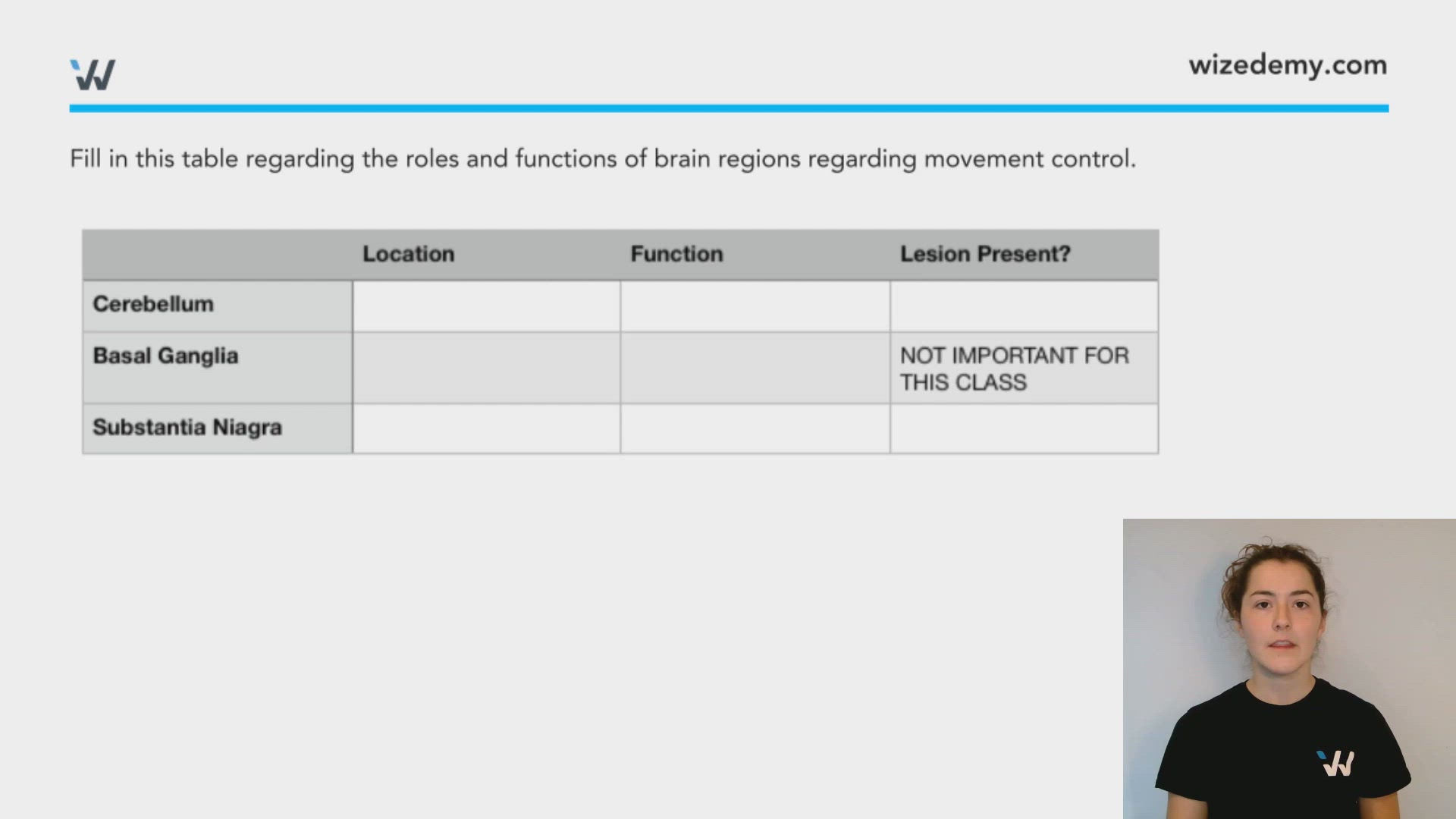
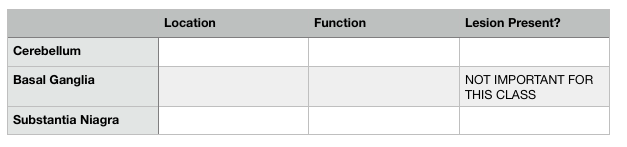
Fill in this table regarding the roles and functions of brain regions regarding movement control.
A patient comes into a clinic and resents with difficulty executing contralateral movements and judging distances. You test your patient for a resting tremor, but there is none present. What might be the diagnosis?